You are here: Urology Textbook > Kidneys > Renal trauma
Renal Trauma: Injury of the Kidney
 |
Renal trauma is an injury to the renal parenchyma, collecting system, or renal vascular system caused by blunt or penetrating external force. Consequences include hemorrhage, ischemia of the renal tissue, or damage to the urinary tract with possible urinary extravasation or urinary outflow obstruction.
Epidemiology and Etiology of Upper Urinary Tract Injuries
Blunt injuries:
Renal injury most commonly results from direct blunt force (compression or contusion), usually in the setting of motor vehicle accidents, falls, or sports injuries. In blunt abdominal trauma, the kidneys are involved in up to 10 % of cases.
Deceleration injury:
Injury to the renal pedicle or ureter, up to and including complete avulsion, caused by the inertia of the renal mass during a fall from a great height or a motor vehicle accident.
Penetrating injuries:
Gunshot or stab wounds are uncommon; they play a greater role in the United States than in Europe. Associated intra-abdominal injuries are common.
Signs and Symptoms of Renal Trauma
Acute signs and symptoms:
- History of abdominal trauma or deceleration injury
- Bruising and hematoma of abdomen or flank
- Abdominal tenderness and tumor
- Flank pain
- Rib fracture
- Hematuria
- Hemodynamic instability, Shock
Late complications of renal trauma:
- Urinoma
- Renal Abscess
- Renal arteriovenous fistula
- Renal hypertension
- Hydronephrosis
- Loss of renal function
Diagnostic Workup of Renal Trauma
Laboratory examinations:
Urine sediment, blood count, creatinine. The lack of hematuria does not exclude severe renal trauma.
%Ultrasound imaging:
Abdominal (renal) ultrasound is a valuable tool for the initial evaluation of abdominal injuries without clear evidence of renal injury. If free abdominal fluid, retroperitoneal hematoma, urinoma, hydronephrosis, or kidney infarction (with Doppler ultrasound) is seen, abdominal CT is necessary for an exact diagnosis.
Computed tomography:
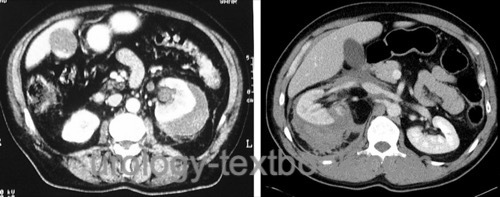
CT scan is the imaging technique of choice if there is a high suspicion of renal injury: severe trauma, abnormalities in ultrasound imaging, or hematuria [fig. CT imaging of renal trauma]. Fill the bladder with contrast medium before CT to exclude bladder injury in blunt abdominal trauma.
Contraindication of CT: patients with hemodynamic instability after initial resuscitation and suspicion for intraabdominal bleeding. They require surgical intervention without further imaging.
 |
Urography (IVP):
Intravenous urography is outdated and has been replaced by computed tomography. IVP may be helpful (as an alternative to CT) to exclude renal injury, e.g., patients with hematuria and normal ultrasound imaging, and if CT is not available. Urography also has a limited role in intraoperative imaging after emergency laparotomy (single shot IVP).
Classification (Severity) Of Renal Trauma
The severity of renal trauma is classified in five grades according to the American Association for the Surgery of Trauma (AAST), see fig. Classification of renal trauma for details.
Treatment of Renal Trauma
Conservative management:
Conservative management is possible in renal trauma with stable circulation and trauma severity grade I–III (no urinary extravasation). Conservative management consists of bed rest until gross hematuria resolves and frequent monitoring of vital signs and blood count. Fever, dropping blood count or flank pain are indications for repeated imaging (ultrasonography or CT) or surgery.
Selective embolization:
Selective embolization is an option in case of persistent bleeding to avoid open surgery.
Internal ureteral stent:
Ureteral stenting is indicated for urinary extravasation in grade IV renal injury (MJ/DJ ureteral stent or percutaneous nephrostomy). Place a urethral catheter to prevent reflux alongside the DJ stent. Large (delayed diagnosed) urinomas are drained percutaneously in addition to ureteral stenting. Antibiotic prophylaxis is often recommended.
Surgical Management:
Indications for surgery:
- Hemodynamic instability after initial resuscitation
- Grade V renal injury with expanding renal hematoma
- Ureteropelvic junction disruption
- Associated intraabdominal injuries
- Gunshot injury
Relative indications (depending on other factors):
- Urinary extravasation with nonviable renal tissue over 25%
- Associated intraabdominal injuries
- Gunshot wounds
- Suspicious intraoperative IVP during emergency laparotomy.
Surgical technique:
Transperitoneal exposure using a midline laparotomy, cell saver and packed red blood cells for transfusion should be ready. Early vascular control (near the aorta) before opening of renal fascia improves renal salvage rate. Renal reconstruction can be done with temporary ischemia. Kidney defects may be sutured (renorrhaphy) and covered with omentum majus, absorbable mesh or retroperitoneal fat. Hemostatic agents help control bleeding tissue. If necessary, insert a nephrostomy for urinary drainage.
Indications for nephrectomy:
- Extensive renal or vascular injury
- Ischemia of the kidney
- Hemodynamic instability due to bleeding
| Medullary sponge kidney | Index | Kidneys |
Index: 1–9 A B C D E F G H I J K L M N O P Q R S T U V W X Y Z
References
Diederichs und Mutze 2003 DIEDERICHS, W. ; MUTZE, S.: [Renal trauma: is open surgery still up to date?].In: Urologe A
42 (2003), Nr. 3, S. 322–7
Kawashima u.a. 2002 KAWASHIMA, A. ; SANDLER,
C. M. ; CORL, F. M. ; WEST, O. C. ; TAMM, E. P. ;
FISHMAN, E. K. ; GOLDMAN, S. M.:
Imaging evaluation of posttraumatic renal injuries.
In: Abdom Imaging
27 (2002), Nr. 2, S. 199–213
R. A. Kozar et al., “Organ injury scaling 2018 update: Spleen, liver, and kidney.,” The journal of trauma and acute care surgery, vol. 85, no. 6, pp. 1119–1122, 2018.
Meria und Mazeman 2000 MERIA, P. ; MAZEMAN, E.:
Immediate and delayed management of renal trauma.
In: Eur Urol
37 (2000), Nr. 1, S. 121–30
Vasile u.a. 2000 VASILE, M. ; BELLIN, M. F. ;
HELENON, O. ; MOUREY, I. ; CLUZEL, P.:
Imaging evaluation of renal trauma.
In: Abdom Imaging
25 (2000), Nr. 4, S. 424–30
 Deutsche Version: Nierentrauma
Deutsche Version: Nierentrauma
Urology-Textbook.com – Choose the Ad-Free, Professional Resource
This website is designed for physicians and medical professionals. It presents diseases of the genital organs through detailed text and images. Some content may not be suitable for children or sensitive readers. Many illustrations are available exclusively to Steady members. Are you a physician and interested in supporting this project? Join Steady to unlock full access to all images and enjoy an ad-free experience. Try it free for 7 days—no obligation.
New release: The first edition of the Urology Textbook as an e-book—ideal for offline reading and quick reference. With over 1300 pages and hundreds of illustrations, it’s the perfect companion for residents and medical students. After your 7-day trial has ended, you will receive a download link for your exclusive e-book.