You are here: Urology Textbook > Surgical Management > Percutaneous nephrostomy
Percutaneous Nephrostomy: Indications, Technique, and Complications
Percutaneous nephrostomy is the image-guided placement (ultrasound and fluoroscopy) of a catheter through the skin and renal parenchyma into the renal pelvis for external urinary drainage.
Indications for Percutaneous Nephrostomy
Percutaneous nephrostomy is an alternative to internal ureteral stenting. The risks and benefits should be assessed on an individual basis.
- Acute obstruction: infected hydronephrosis, especially with urosepsis or pyonephrosis. For any hydronephrosis if retrograde stenting fails.
- Chronic obstruction: advanced tumors with ureteral compression, retroperitoneal fibrosis (Ormond disease), or ureteral strictures, especially if ureteral stenting fails.
- Perioperative: percutaneous renal procedures (PNL), rarely in open surgical operations (renal trauma, complex pyeloplasty, or partial nephrectomy).
- Bladder decompression: palliative unilateral or bilateral percutaneous nephrostomy for urinary fistulas, or bladder dysfunction due to tumor infiltration.
- Diagnostics (rare): antegrade pyeloureterography, Whitaker test (measuring renal pelvic pressure), and split renal function assessment.
Contraindications
Absolute contraindications are severe, uncorrectable coagulopathies. Relative contraindications include malignant renal tumors, high risk or technical difficulties of percutaneous puncture (absence of hydronephrosis, severe obesity, anatomical variations, uncooperative patient).
Different Forms of Nephrostomy Catheters
For long-term indications, the nephrostomy catheter must be changed regularly, every 6–12 weeks, depending on the frequency of recurring obstructions or infections.
- Pigtail catheter: a single-lumen catheter with a coiled tip, usually made of polyurethane. Placement is technically straightforward, as the accompanying dilator system facilitates insertion into the renal pelvis. The catheter requires skin fixation with a suture. Available in sizes 6–12 Ch.
- Locking-loop catheter: a modern variant of the pigtail catheter. A locking suture mechanism secures the loop configuration, providing a more stable positioning within the renal pelvis.
- Balloon catheter: a double-lumen silicone catheter with a retention balloon and a short, centrally open tip. Balloon catheters are particularly suitable for long-term drainage, as they require no skin sutures. Available in sizes 10–24 Fr.
- Malecot catheter: a single-lumen catheter made of silicone or polyurethane. After removal of the inner stylet, a mushroom-shaped tip with wings expands, anchoring the catheter in the renal pelvis. Additional skin suture fixation is necessary. Malecot catheters are outdated and rarely used today.
Technique of Percutaneous Nephrostomy
- Patient positioning: Place the patient in the prone position if stable to allow a comfortable puncture. Consider the lateral or supine position for unstable patients, although the puncture becomes technically more challenging.
- Initial puncture: Perform an ultrasound-guided puncture of a lower or middle calyx using a hollow needle. Confirm correct needle placement by observing urine drainage and performing antegrade pyelography. Conduct all subsequent steps under continuous fluoroscopic guidance.
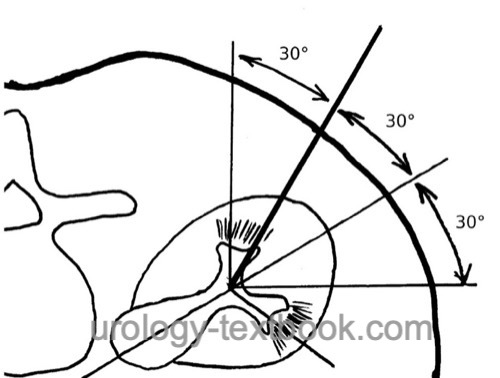
- Guidewire placement: Advance a stiff guidewire (Lunderquist wire) into the renal pelvis. Use the posterior calyx group to easily access the renal pelvis. In the prone position, angle the needle 20–30 degrees laterally from vertical [Fig. calyx puncture]. For long-term nephrostomy, select a puncture site as lateral as possible to prevent pressure on the nephrostomy during sleep.
- Tract dilation and catheter insertion: Dilate the nephrostomy tract along the guidewire, then advance the nephrostomy catheter (initially 8–12 Ch) into the renal pelvis.
- Catheter fixation: Secure the nephrostomy with a suture and apply a sterile dressing.
 |
Complications of Percutaneous Nephrostomy
- Acute complications: bleeding, renal pelvis tamponade, perforation of the renal pelvis, infection up to urosepsis, and very rarely injury to adjacent organs (pneumothorax, colon, duodenum, liver, spleen).
- Long-term complications: nephrostomy obstruction, infection/urosepsis, catheter dislodgement or loss, urine leakage from the nephrostomy tract, skin irritation.
| Intermittent catheter | Index | Pharmacology |
Index: 1–9 A B C D E F G H I J K L M N O P Q R S T U V W X Y Z
References
Ahmad MU, Siddiqui S, Ashraf FA, Iqbal R, Ehsanullah SAM, AlFayadh A, Siddiqui MRS, Khan MS, Furrer MA. Retrograde Ureteral Stents Versus Percutaneous Nephrostomy in the Management of Malignant Ureteral Obstruction: A Systematic Review and Meta-Analysis. Urology. 2024 Oct;192:158-167. doi: 10.1016/j.urology.2024.05.042.
Cardoso A, Coutinho A, Neto G, Anacleto S, Tinoco CL, Morais N, Cerqueira-Alves M, Lima E, Mota P. Percutaneous nephrostomy versus ureteral stent in hydronephrosis secondary to obstructive urolithiasis: A systematic review and meta-analysis. Asian J Urol. 2024 Apr;11(2):261-270. doi: 10.1016/j.ajur.2023.03.007.
 Deutsche Version: Indikationen und Komplikationen der perkutanen Nephrostomie
Deutsche Version: Indikationen und Komplikationen der perkutanen Nephrostomie
Urology-Textbook.com – Choose the Ad-Free, Professional Resource
This website is designed for physicians and medical professionals. It presents diseases of the genital organs through detailed text and images. Some content may not be suitable for children or sensitive readers. Many illustrations are available exclusively to Steady members. Are you a physician and interested in supporting this project? Join Steady to unlock full access to all images and enjoy an ad-free experience. Try it free for 7 days—no obligation.
New release: The first edition of the Urology Textbook as an e-book—ideal for offline reading and quick reference. With over 1300 pages and hundreds of illustrations, it’s the perfect companion for residents and medical students. After your 7-day trial has ended, you will receive a download link for your exclusive e-book.