You are here: Urology Textbook > Surgery (procedures) > Ureteroureterostomy
Ureteroureterostomy: Surgical Technique and Complications
Reteroureterostomy is the end-to-end anastomosis of the ureter, which can be performed with open surgery, laparoscopy, or robotic-assisted laparoscopy for the following indications: (Elliot and McAninch, 2006).
Indication for Ureteroureterostomy
- Ureter injury
- Treatment of short segment (<3 cm) ureteral stricture of the middle and proximal ureter. Prefer the reimplantation of the ureter for distal ureteral strictures.
- Treatment of retrocaval ureter
 |
Contraindications
- Coagulation disorders.
- Long ureteral stricture or ureteral defects not allowing a tension-free end-to-end anastomosis.
- Kidneys without sufficient function (<15% of total glomerular filtration rate)
- Further contraindications depend on the surgical risk due to the comorbidity of the patient, the renal function of the contralateral kidney and the impact of the surgical procedure on the quality of life of the patient.
Surgical Technique of Ureteroureterostomy
Preoperative Patient Preparation
- Exclude or treat urinary tract infection
- Perioperative antibiotic prophylaxis
- Retrograde pyelography to confirm the diagnosis and length of the ureteral defect. Insert a DJ ureteral stent (if possible).
- Transurethral catheter
Surgical Approach
The surgical approach to the proximal ureter is via a flank incision. The mid-ureter and distal ureter are reached with a retroperitoneal or transperitoneal lower abdomen incision, e.g., paramedian laparotomy or Gibson incision. A laparoscopic (robotic-assisted) approach is also possible. After identification, mark the ureter with a vessel loop and continue to mobilize the ureter cranial and caudal to the stricture. It is essential to treat the ureter atraumatically and to spare its vascular supply.
Anastomosis of the Ureter:
- Identify the stricture or injury and remove the diseased part of the ureter. Consider frozen section examination if malignancy is possible. Both ends of the ureter must be free of scarred tissue, have a good vascular supply, and be brought together without tension.
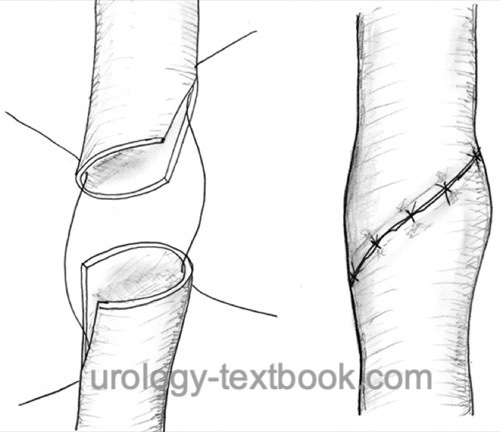
- The proximal and distal end are spatulated about 7–10 mm at 180 degrees apart.
- Sometimes, complete mobilization of the kidney is necessary to obtain sufficient ureteral length for tension-free anastomosis.
- Insert a ureteral stent, if you have not done preoperatively.
- Place corner sutures (e.g., PDS 5-0). Complete the ureteral anastomosis using the corner sutures or in an interrupted fashion [fig. ureteroureterostomy].
- Insert a wound drainage near the ureteral anastomosis.
- Wound closure
Postoperative Care after Ureterureterostomy
General Measures:
Early mobilization, thrombosis prophylaxis, respiratory therapy, laboratory tests (hemoglobin, creatinine), regular physical examination of the abdomen and incision wound.
Analgesia:
Analgesics with a combination of NSAIDs and opioids. Peridural anesthesia facilitates postoperative pain management.
Drains and Catheters:
Remove the retroperitoneal drainage if the daily drainage is below 50 ml. The bladder catheter stays additional 1–2 days or 3–5 days in total, and the ureteral stent for 2–4 weeks.
Complications of Ureteroureterostomy
Bleeding, infection, urinoma, recurrent ureteral stricture, loss of kidney function, injury to adjacent organs (bowel, liver, spleen, pancreas).
| Laparoscopic pyeloplasty | Index | Ureteral reimplantation |
Index: 1–9 A B C D E F G H I J K L M N O P Q R S T U V W X Y Z
References
Elliott, S. P. & McAninch, J. W.
Ureteral
injuries: external and iatrogenic
Urol Clin North Am, 2006,
33, 55-66, vi
 Deutsche Version: Ureteroureterostomie
Deutsche Version: Ureteroureterostomie
Urology-Textbook.com – Choose the Ad-Free, Professional Resource
This website is designed for physicians and medical professionals. It presents diseases of the genital organs through detailed text and images. Some content may not be suitable for children or sensitive readers. Many illustrations are available exclusively to Steady members. Are you a physician and interested in supporting this project? Join Steady to unlock full access to all images and enjoy an ad-free experience. Try it free for 7 days—no obligation.
New release: The first edition of the Urology Textbook as an e-book—ideal for offline reading and quick reference. With over 1300 pages and hundreds of illustrations, it’s the perfect companion for residents and medical students. After your 7-day trial has ended, you will receive a download link for your exclusive e-book.