You are here: Urology Textbook > Penis > Peyronie disease > Causes
Peyronie disease: Causes and Symptoms
- Peyronie disease: Epidemiology and causes
- Peyronie disease: Diagnosis and treatment
Definition of Peyronie disease
Peyronie disease (PD) is an acquired fibrosis of the tunica albuginea, which may be accompanied by pain, penile deviation or deformity, erectile dysfunction and distress. PD is also called Induratio penis plastica.
Epidemiology of Peyronie disease
An increasing prevalence rate with age is reported: 30–39 years (1.5%), 40–59 years (3%), 60–69 years (4%) and over 70 years (6.5%). The symptomatic prevalence is approximately 1% for all age groups. The prevalence of Peyronie disease at autopsy is much higher, with up to 20% penile indurations.
Causes (Etiology) of Peyronie disease
Microtrauma and Peyronie disease
Trauma (Bending) of the penis is a risk factor for Peyronie disease. More frequent and vigorous sexual intercourse is a risk factor, and sexual intercourse in positions which are potentially traumatic to the penis. The manifestation of Peyronie disease represents a pathological form of wound healing of the tunica albuginea.
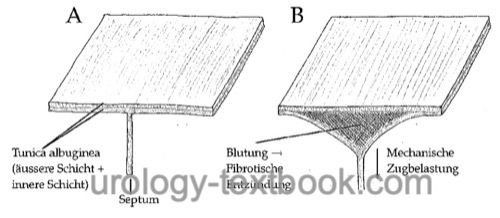
The tunica albuginea of the corpora cavernosa consists of two layers (outer longitudinal and inner circular layer). Due to traumatic events (see above), these two layers are separated, most likely at the septal insertions. The delamination of the tunica albuginea leads to bleeding and clot formation. Macrophage invasion creates a fibrotic inflammatory response by releasing growth factors (e.g., TGF-β). The fibrotic inflammatory response can maintain itself and lead to the formation of a penile deviation with fibrotic plaques.
 |
Associated Diseases and Conditions
The following diseases or conditions are associated with Peyronie disease: Dupuytren disease (30–40%), Ledderhose disease (plantar form of Dupuytren disease), liver cirrhosis, rheumatic diseases, tympanosclerosis, penile or urethral trauma, urethral instrumentation, urethritis, diabetes mellitus, Paget disease, treatment with β-blocker (weak evidence).
Erectile Dysfunction and Peyronie disease
Penile plaques destroy the elasticity of the tunica albuginea and thus lead to erectile dysfunction due to venous insufficiency. A pronounced penile deviation is a mechanical handicap for vaginal penetration and causes psychological frustration. Circular plaques can cause instability of the penis.
Pathology of Peyronie disease
The deposition of fibrin is typical in penile plaques due to Peyronie disease. Fibrin usually is absent in scar tissue of the tunica albuginea. Furthermore, the plaques consist of dense connective tissue with collagens, and the elastin is fragmented and diminished. The expression of TGF-β is increased. Neighboring vessels show infiltrates with lymphocytes. In 30%, dystrophic calcifications of the plaques are found.
Signs and Symptoms of Peyronie disease
Peyronie disease often shows two stages:
- Inflammatory stage: palpable induration, painful erection and increasing deviation. The pain usually improves within six months.
- Stable disease: static deviation and often erectile dysfunction.
Penile Deviation
The penile deviation may show a dorsal, lateral or ventral curvature. A pronounced deviation prevents sexual intercourse. The curvature is often associated with penile shortening.
Penile Plaques
The penile plaques are palpable on the concave side of the deviation in the tunica albuginea of the corpora cavernosa.
Natural History of Peyronie disease
In up to 15%, Peyronie disease shows a spontaneous regression. In 40%, the disease remains stable. The following factors make a spontaneous regression unlikely: penile deviation over 45 degrees, disease duration over two years, plaque calcification, or concurrent Dupuytren disease.
| Erectile dysfunction | Index | Peyronie disease |
Index: 1–9 A B C D E F G H I J K L M N O P Q R S T U V W X Y Z
References
A. Nehra et al. “AUA Guideline: Peyronie’s Disease,” 2015. [Online]. Available: https://www.auanet.org/guidelines-and-quality/guidelines/peyronies-disease-guideline.
EAU-Guidelines: Sexual and Reproductive Health
Gholami u.a. 2003 GHOLAMI, S. S. ;
GONZALEZ-CADAVID, N. F. ; LIN, C. S. ; RAJFER,
J. ; LUE, T. F.:
Peyronie’s disease: a review.
In: J Urol
169 (2003), Nr. 4, S. 1234–41
Hauck, E. W. u. a. (2006). A critical analysis of nonsurgical treatment of Peyronie’s disease. In: Eur Urol 49, S. 987–997.
Nesbit 1965 NESBIT, R. M.:
Congenital Curvature of the Phallus: Report of Three Cases with
Description of Corrective Operation.
In: J Urol
93 (1965), S. 230–2
Tunuguntla 2001 TUNUGUNTLA, H. S.:
Management of Peyronie’s disease-a review.
In: World J Urol
19 (2001), Nr. 4, S. 244–50
Yachia 1990 YACHIA, D.:
Modified corporoplasty for the treatment of penile curvature.
In: J Urol
143 (1990), Nr. 1, S. 80–2
 Deutsche Version: Ursachen der Induratio penis plastica (Morbus Peyronie)
Deutsche Version: Ursachen der Induratio penis plastica (Morbus Peyronie)